



Looking Beyond the Mental Health Industrial Complex for Answers
A key principle that guided our forthcoming book.

Dialog – Debate – Discuss
We wrote a book about the state of adolescent and young adult mental health. It took Will Dobud and I about 18 months. It was a lot of work, but also very interesting, rewarding and insightful for us both as we shared beliefs and challenged each other with our individual perspectives on the world. We finally agreed to use Oxford commas, not pull our punches on some issues, and that we likely have some differing perspectives still to be hashed out. All good.
Our book’s sales handle is: An unflinching exploration of how interference, intervention, and ideology are harming youth mental health and development
As our book is about ‘kids these days,’ and we are both therapists, we discussed and wrote about mental health, a lot. We do agree that we live in a time of over-diagnosis (including self-diagnosis which will be the topic of a future post), over-medication and over-protection. The stats are scary and include a solid trail of evidence suggesting we have now the most mentally ill generation ever!
**But those are numbers, and not kids.**
Will and I shared knowledge (dialog), argued a bit (debate) and examined issues closely and broke down what we found (discussion). While not always aware of which mode we were operating with, we valued the range of approaches we took to each topic we covered in the book. Sometimes it’s more important to listen and ponder, at other times it seems worthwhile to push back. Most vital was, we had to write it down.
This process has allowed each of us to reflect and grow in our understanding of what is going on with youth mental health, but also to recognize there are no absolute truths. That is one thing we agreed upon early and is the same reason why we rally against quick-fix, universal or “10-easy-step” solutions proposed for the issues young people face today.
“It’s the phones!” Yes Jonathan, and… “It’s over therapizing kids!” Yes Abigail, and… “It’s a lack of outdoor childhood play!” Yes Lenore, and, there is much more affecting kids today than just those three factors. That was the genesis of our book—that it is a multi-variable problem. And we promised to NOT write a sensationalist, media and attention-grabbing, and offer of cure, to all that ails our youth today. We also promised to NOT write another parenting book. We ended up writing for adults who care about kids, hopefully that is all of them. We should see it in bookstores by end September 2025 (with online pre-sales in February we are told). In the meantime, we plan to dive into these topics in other forums, this Substack being one of them.
We also invite further dialog, debate, and discussion. The comments section will be open. Please use respectfully:)
Healthcare is an Industry
While modern Western history points to ancient Egypt and Greece as the birthplace of diagnosing illness, its likely every society had a practice of pointing out what was wrong with us. Before testing was done, the ‘healers’ had only symptoms to go on. What we experience in modern psychology, is in many ways, quite similar. Symptoms, often self-reported, are the principal factors in diagnosing. While usually only the domain of MDs, Psychiatrists, Clinical Psychologists and some other licensed practitioners, these folks rely primarily on reports from the individual being assessed.
Historically, the healers then provided treatments for each diagnosis, whatever may have been the flavour of the day. From exorcisms to smoke enemas, to electrical charges to lobotomies and hysterectomies, the treatments have changed over the years while many of the issues and chief complaints remain the same. On that, and something we talk about often and will write about more, is how psychotherapy hasn’t made much progress since its first inception! Today, we know anxiety and depression are the two most common conditions in Western societies. We also know young adults and teens leading cause of death is suicide, and this is highly troubling and needing more attention.
What we have in response to the crisis in mental health is the medical model. Surgical and pharmaceutical. The two big tools of modern medicine are readily available and most often employed. Both have significant financial implications for the providers, manufacturers, and stakeholders gambling on profit margins. This is big business. With any for-profit business, efficiencies and volume are the common goals. The problem with this model in health and human services is that those being served become collateral damage, where care and compassion for individual needs and differences are hardly ever considered. This is not a new argument. For a solid critique of the medical model of mental health, see Thomas Szaz’s 1961 Myth of Mental Illness
So, is the realm of mental healthcare an industry? I argue yes. More so stateside, but we Canadians experience a similar effect. And is this industry one susceptible to corruption or questionable ethics in practice? Again, of course it is. Pharmaceutical sales, assessment services, treatment provision, and the billing of practitioners to private insurance companies or out-of-pocket payments by those served all leads to the potential for corruption and less than quality practice. Competition and the capitalistic market can be beneficial to drive new products and services to the consumer. Health and human services also have healthcare providers operating as for-profit entities, with influence from lobbyists and political influencers, and often a complex billing system that creates a massive administrative overhead cost to be absorbed by the consumer—often the person incapacitated by health concerns. In short, costs are driven up, and people are left with inadequate care due to the financial burden or lack of accessible services. Again, maybe less so in Canada due to levels of provision of public healthcare.
In short, the over-medicalization of the human condition has left us with a system which is vulnerable to valuing profit over care and increases inequity and access across populations. Further, much of mental health is based on ideas in psychology versus material evidence, such as biological or measurable changes in our bodies or minds. You cannot conduct a biopsy for grief! This is one clear distinction between mental health and health, although often spoken of in the same breath by the healthcare industry.
Mental Health Specifically
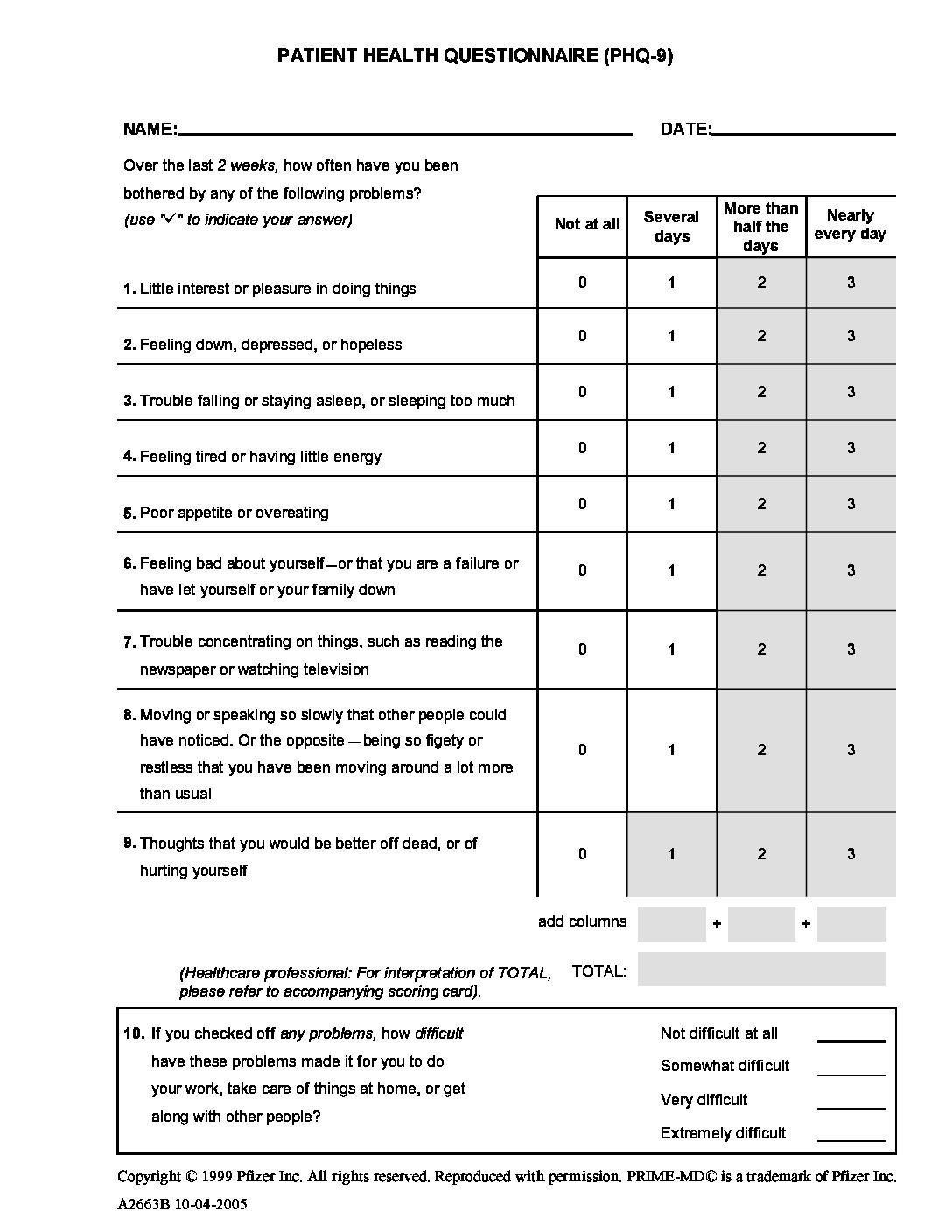
A mental health diagnosis is a subjective, most often self-described and reported set of feelings, behaviors and beliefs. I am not saying mental health problems are not real. A diagnosis is quite reliant on an individual’s ability to articulate emotions, thoughts and in providing answers to standardized questionnaires. Introducing the book, Will and I pick at one mental health measure commonly used for diagnosing depression and anxiety today, the PHQ-9. I’ll only briefly recap here: 9 questions given by physician to patient, self-reported answers, score tallied, diagnosis made, medications prescribed, in the average 10-minute doctor’s office visit.
Consider Question 3 below. Over the last two weeks, how often have you been bothered with trouble falling asleep or staying asleep, or sleeping too much? Does a question like this capture much context? Which is worse? Too much sleep? Too little? Then one gets to the subsequent question, too much energy? Or too little? The physicians who needed the measures to diagnose anxiety and depression, are not privileged with time to inquire between questions, take notes, or contextualize their patient’s responses.
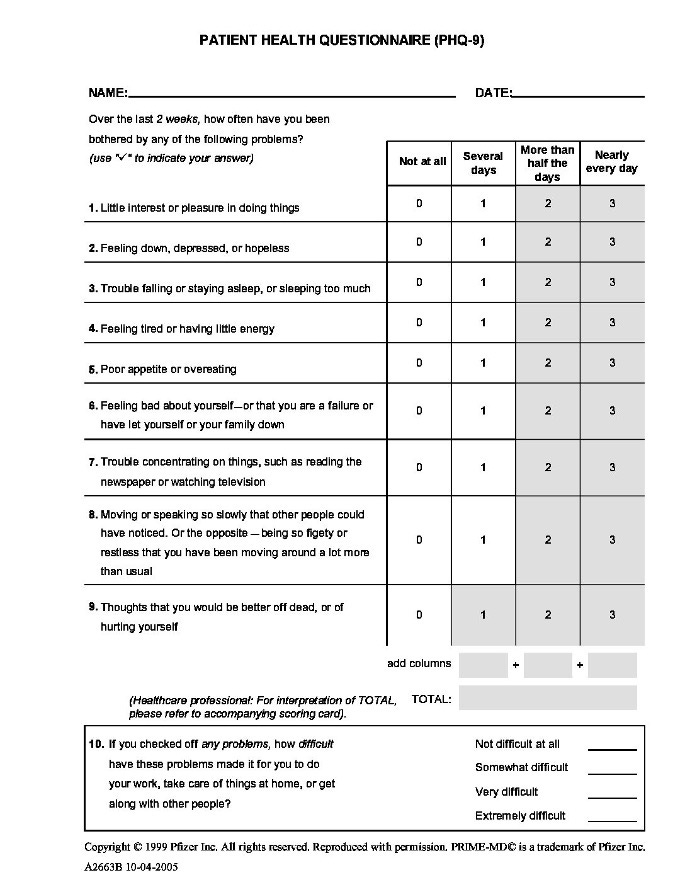
Figure 1: Patient Health Questionnaire (PHQ-9) Retrieved from USC.
{kind=link}
Does this sound like a recipe for success? What does the physician have time to learn about the person in their office? What do they know about their health, family, current events in their life? The PHQ-9 has 2 questions to diagnose anxiety, and 7 for depression. Following the scoring a patient is found to land in one of 5 categories from non-minimal to severe. Pharmaceuticals are considered for 3 of the 5 categories along with recommendations for therapy.
Not to be critical of the physicians here. They asked for the tools to be able to help those with anxiety and depression. Problem is the measures were manufactured by the marketing team of the same folks who make the meds to proscribe based on your scores. Bit of conflict of interest there, no?
And if we want to get straight about factors leading to a youth mental health crisis, we need to include in our analysis the dates that scales like the PHQ-9 were put into play. 1999 in this case. And what impact did the measures have on rates of reported depression and anxiety? We read with interest James Davies’ critique in his book Sedated, and promise to cover this topic more thoroughly as it relates to rates of mental health diagnoses.
Don’t Trust the Experts, say the Experts
Reliance on ‘experts’ has become the norm today. Knowledge is highly reductionist and puts many in ‘lanes’ which we are supposed to stay in. We don’t adhere to the principal but also don’t talk out of our asses. If we don’t know, we own that. If we have enough evidence to make a claim, we will also try to keep our brave pants on and share it out loud.
Funny thing happened on the way to writing Kids These Days…our experts told us “Don’t trust the experts!” What they meant is easily understood when you look at the quality and integrity of meaningful available research and then learn it takes years to decades before it translates to policy or meaningful change. In 2011, one study suggested the research to practice lag was about 17 years! This delay is brutal, especially in healthcare. We’d hope knowledge translation with modern methods of dissemination have reduced this. Systems can be uncooperative, even aggressively defending bad practice and/or bad medicine. We have first-hand experience with this in outdoor therapies, a topic we will tackle in a future post to better flesh out the details as an example of system-level issues and compromised ethics in practice.
Overall, the mental health industrial complex (some have labelled and defined it) perpetuates and feeds on the myth of individual pathology. Consider this belief system driving the design of diagnostic measures, the medication, the care and treatment systems and their intricate inter-relationships as the ‘complex.’
Krishnamurti famously said, “It is no measure of health to be well adjusted to a profoundly sick society” and suggested societal and systemic issues are more likely causes of mental health issues than something defective in one’s brain. This is quite obvious, and most in social and human services knows this. Environmental conditions, whether social, emotional, physical, spiritual, economic, or otherwise have significant impacts on how we feel, what we think and our behaviours in response.
How can young people today be mentally well if all they hear is of collapsing democracies, failing economic systems, environmental catastrophes and the details of the latest school shooting? A child living in a community where drug abuse and violence is rampant is diagnosed with depression and medicated. They move to a relative’s home where the home and community are healthy and vibrant. They no longer need their meds. Where is the depression? Did it leave the child’s brain? Was it in their bones? This is simplifying and not meant to be cavalier with issues like depression. The point is that mental illness has been more than once critically been called a myth when compared directly to physical ailments or disease which can be seen, measured and treated directly.
Let’s not be Overly Dramatic
On a less sensationalist level, youth today are inundated with social media, technological advancements like ChatGPT and more entertainment than any of us can handle. Kids in decades past, and the adults, had to adapt to radio, television, rock and roll, gaming, the internet and now infinite scrolls, like buttons and the evil ‘algorithm.’ Most of us adapted and worked through the changes in technology and went on to be productive adults.
We interviewed the author of I-Minds, Dr. Mari Swingle and she shared her perspectives on social media and the role of the e-devices in kids’ lives. Can they be harmful? Sure. Can we live our lives integrated with technology? Sure. While developing, children have little hope of keeping up and adapting in a healthy way to the volume and type of content available to them on screens. That is where the adults come in. To set boundaries, to teach and role model behaviors, and to limit, when necessary, kids access and use of devices. We’ll revisit screens and technology in a future post specifically, but for now, we can leave you with a hopeful message from a non-sensationalist level-headed expert about screen addiction and developmental concerns. Dr. Swingle is clear that it’s about developing digital integration and avoiding digital interference. This is the adult’s job to help kids grow through the process of learning self-regulating behaviors related to use.
Calming the Moral Panic
What we’ve witnessed lately is a new moral panic. We see kids labelled as the anxious generation. We see adults pushing for governments and schools to enforce mandates, such as “bell-to-bell” device bans in schools. Again, we’ll come back to this topic more fully, talk to some experts, and share what we find. We do know that universal measures are doomed to fail, even if short-term success feels right. We see it again and again. We have worked with kids with developmental differences that excel at school because they have support devices. We have seen youth who are ok at school with their anxiety because they have access to text a parent or sibling. And we know educators who have embraced technology in ways that students can use their devices to interact with curriculum, often making lifeless content come to life. These examples are all eliminated when an all-school ban on devices is levied against youth. Regrettable substitutions will surface.
One example, from my 17-year-old daughter’s high school, has imposed the cell phone ban upon the entire school (~1000 students in grade 8-12). Some teachers have gone “over the top” enforcing it, in some cases compromising teacher-student relationships, while other teachers have ignored the edict. Some students are finding other workarounds by either sneaky behavior or getting accommodations for device use in classrooms that teachers then have to honour while trying to prevent others from using them. All the while, tech companies continue their unscrupulous behaviours, knowing the addictive nature of their products and exploiting children and youth for profit.
The adults in the room should be focusing their energies on the corporations profiting on easily addictive apps and features, adulting in ways to reduce screentime rather than applying universal bans on devices. If 1 in 4 youth today have a mental health condition, and some blame the phones directly, then why are 3 in 4 having the ban applied to them too?
A View from 40,000 Feet
Our book Kids These Days questions the mental health crisis of youth. We know the ‘crisis’ is not in youth but rather happening to youth. The stats are horrific, and issues need to be addressed. We understand that fully as practitioners, researchers and parents. We framed our book as an unflinching critique of current issues for youth and how many interventions are simply based on bad theory (ideologies) or simply interfering in child and adolescent growth and development.
Kids These Days back cover text: Examining everything from social media, overprotection, and environmental toxins to the erosion of connection and failings of the mental health industry, Kids These Days draws on cutting edge research and casts a critical eye on the adolescent mental health crisis and presents solutions for raising healthy youth. We basically want to get beyond hearing only about mental health as its measured and described by the mental health industry. That is not a statement intended to offend anyone. I am a part of it. I have been an educator and mentor of mental health professionals. I see clients with diagnoses and medications. I still recognize the system I work in, and want to explore and question what we are doing. With more youth diagnosed and medicated than ever, maybe we need more questions than defences.
Will and I wrote about what is harming kids but are directing our call to action toward the adults, hence, here we are introducing this Substack, Adults in the room. A podcast format is in the works too!
Future topics
We aim to cover the topics we wrote about in Kids these Days, and many we couldn’t fit in. We are also open to hearing from you about topics you are curious about and where you believe there are, or needs to be, more adult sin the room addressing the issues.
Some future posts may include…
-Medicalization of adolescence.
-How psychotherapy hasn’t changed in more than a century.
-How shockingly obvious some youth mental health issues and resolutions are.
-Regrettable substitutions.
-The attention economy.
-Overprotection in our risk-averse society.
-Environmental toxins and child development.
Be well,
Nevin
